
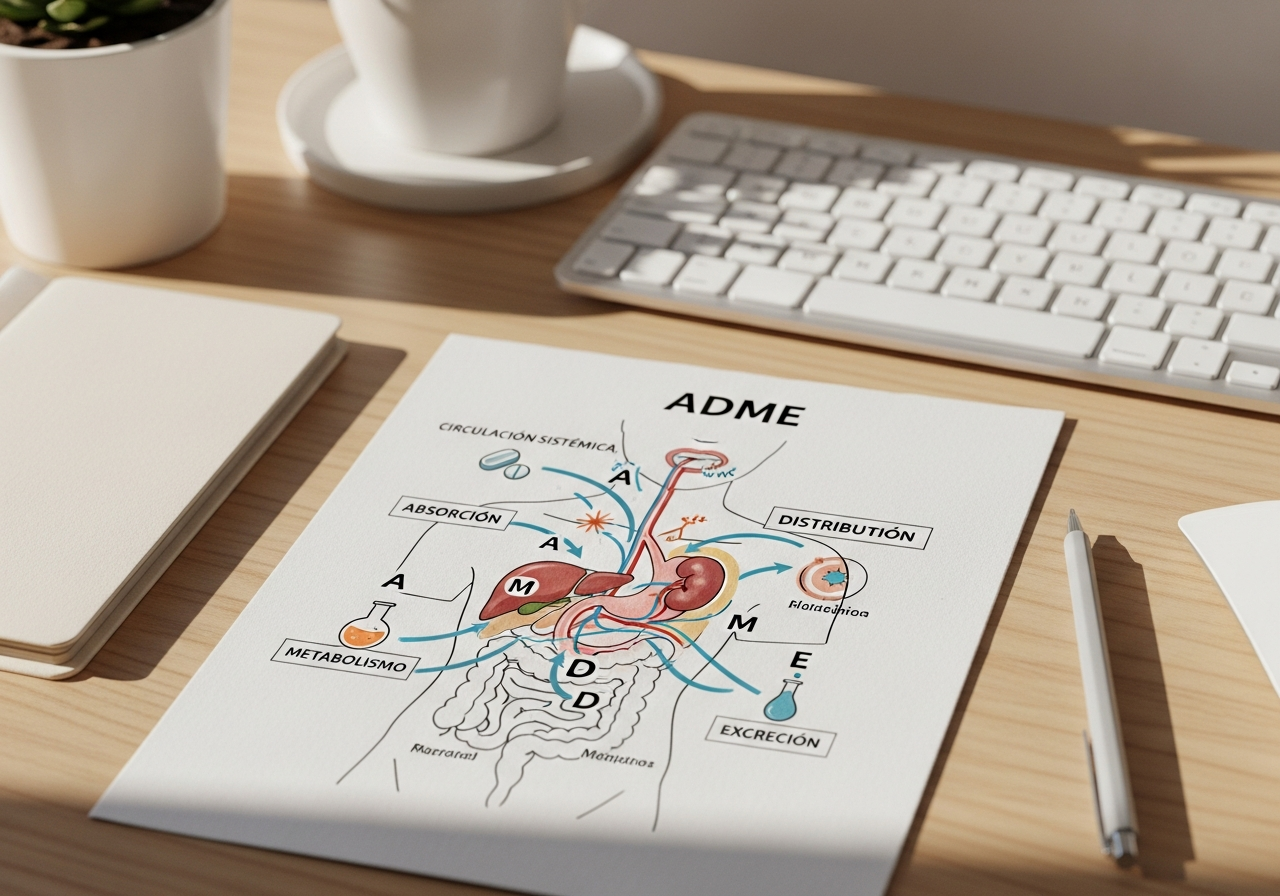
Pharmacology Quiz: Key Questions on Pharmacokinetics (ADME)
Hey, future doctor. We know that pharmacokinetics can be one of the toughest nuts to crack in your 3rd year of med school. Concepts like volume of distribution, clearance, or zero-order kinetics can seem abstract and hard to apply. But the key to mastering them isn't rereading your notes over and over, but actively testing yourself (a technique known as Active Recall). This practice exam is designed for exactly that: to help you identify your strengths and, more importantly, your weaknesses before the big day. Let's get to it!
Test Yourself: Pharmacokinetics (ADME) Quiz
1. A drug administered orally has a bioavailability of 50%. What is the most likely cause of this incomplete bioavailability if we know it is completely absorbed in the intestine? a) High binding to plasma proteins. b) Extensive first-pass hepatic metabolism. c) Low lipid solubility of the drug. d) Rapid renal elimination without being metabolized.
2. A patient receives a drug with an apparent Volume of Distribution (Vd) of 400 L. What is the clinical implication of this value? a) The drug is distributed mainly in the vascular compartment. b) The drug accumulates extensively in peripheral tissues. c) The drug is rapidly eliminated by the kidney. d) The drug has low binding to plasma proteins.
3. A patient on chronic treatment with warfarin (an anticoagulant) starts taking rifampicin (an antibiotic). What effect would you expect on the action of warfarin? a) Increased anticoagulant effect due to enzyme inhibition. b) Decreased anticoagulant effect due to induction of cytochrome P450. c) No effect, as they act through different mechanisms. d) Increased anticoagulant effect due to displacement from protein binding.
4. In a case of poisoning by a weak acid drug, like acetylsalicylic acid, what measure would promote its renal elimination? a) Acidification of urine with ammonium chloride. b) Alkalinization of urine with sodium bicarbonate. c) Administration of a loop diuretic like furosemide. d) Decrease in plasma pH.
5. Which of the following drugs is characterized by following zero-order elimination kinetics at therapeutic doses? a) Paracetamol. b) Amoxicillin. c) Phenytoin. d) Morphine.
6. After starting treatment with a drug administered by continuous infusion, approximately how many elimination half-lives (t½) are needed to reach 94% of the steady-state concentration? a) 1 half-life. b) 2 half-lives. c) 4 half-lives. d) 7 half-lives.
7. If drug A has a total clearance greater than that of drug B, but both have the same volume of distribution, what can we say about their elimination half-life (t½)? a) The t½ of drug A will be longer than that of B. b) The t½ of drug A will be shorter than that of B. c) The t½ of both drugs will be identical. d) The relationship cannot be determined without knowing the dose.
8. A drug has 99% plasma protein binding. What is a direct consequence of this? a) Its volume of distribution will be very large. b) Only 1% of the drug is pharmacologically active and can diffuse into tissues. c) Its elimination will be exclusively via the biliary route. d) The free fraction of the drug is very high.
9. Which of the following administration routes completely avoids the first-pass hepatic effect? a) Oral. b) Rectal (partially). c) Intravenous. d) Intramuscular.
10. Glucuronidation is a key metabolic process for many drugs. To which phase of metabolism does it belong and what is its main objective? a) Phase I, its objective is to introduce a reactive functional group. b) Phase II, its objective is to increase the water solubility of the compound to facilitate its excretion. c) Phase I, its objective is to oxidize the drug via CYP450. d) Phase II, its objective is to activate the drug so it can bind to its receptor.
How did it go? The reasoned answers are below. If you missed more than 3, you need to review your notes. Pharmacokinetics is unforgiving and is fundamental to clinical practice. Don't worry, you still have time to master it!
Answers and Explanations
1. Correct answer: b) Extensive first-pass hepatic metabolism.
- Explanation: Bioavailability is the fraction of the drug that reaches the systemic circulation unchanged. If it's well absorbed in the intestine, the main cause of a drastic reduction is presystemic or "first-pass" metabolism, where the drug passes through the liver (via the portal vein) and is metabolized before being distributed throughout the body.
2. Correct answer: b) The drug accumulates extensively in peripheral tissues.
- Explanation: The Volume of Distribution is a theoretical value that relates the total amount of drug in the body to its concentration in plasma. A Vd much higher than the total body water (approx. 42 L) indicates that the drug is not in the blood, but has been distributed and "sequestered" in tissues like adipose or muscle.
3. Correct answer: b) Decreased anticoagulant effect due to induction of cytochrome P450.
- Explanation: Rifampicin is a potent inducer of several cytochrome P450 (CYP) enzymes. By inducing warfarin's metabolism, it accelerates its elimination, decreasing its plasma levels and, therefore, its anticoagulant effect. This can lead to a risk of thrombosis.
4. Correct answer: b) Alkalinization of urine with sodium bicarbonate.
- Explanation: This is a classic example of "ion trapping." By alkalinizing the urine, a weak acid drug (like ASA) becomes ionized (A-). In its ionized form, it cannot be reabsorbed through the renal tubules, getting "trapped" in the urine and promoting its excretion.
5. Correct answer: c) Phenytoin.
- Explanation: Zero-order kinetics means that a constant amount of drug is eliminated per unit of time because the elimination mechanisms are saturated. Phenytoin, ethanol, and acetylsalicylic acid (at high doses) are the classic examples.
6. Correct answer: c) 4 half-lives.
- Explanation: This is a fundamental pharmacokinetic rule. It is considered that a steady state is reached after approximately 4-5 half-lives. After 1 t½, 50% is reached; after 2 t½, 75%; after 3 t½, 87.5%; and after 4 t½, 93.75%.
7. Correct answer: b) The t½ of drug A will be shorter than that of B.
- Explanation: The relationship is: t½ ≈ (0.693 * Vd) / Cl. If the Vd is the same, the half-life (t½) and clearance (Cl) are inversely proportional. Greater clearance (more efficient elimination) means a shorter half-life.
8. Correct answer: b) Only 1% of the drug is pharmacologically active and can diffuse into tissues.
- Explanation: Plasma proteins (like albumin) act as an inactive reservoir. Only the free (unbound) fraction of the drug can distribute to tissues to exert its effect and be eliminated. High binding limits the amount of available drug.
9. Correct answer: c) Intravenous.
- Explanation: The intravenous route introduces the drug directly into the systemic circulation, so its bioavailability is 100% by definition, and it completely avoids passing through the liver before distribution. The intramuscular and rectal routes also largely avoid it, but not 100%.
10. Correct answer: b) Phase II, its objective is to increase the water solubility of the compound to facilitate its excretion.
- Explanation: Drug metabolism has two phases. Phase I (oxidation, reduction, hydrolysis) introduces functional groups. Phase II (conjugation) joins an endogenous molecule (like glucuronic acid) to the drug, creating a much larger, more polar, and water-soluble compound that is easily excreted by the kidney or in bile.
Where Students Usually Go Wrong in Pharmacokinetics (ADME)
- Confusing Volume of Distribution (Vd) with a real volume: Many fall into the trap of thinking that a Vd of 400 L is a physiological space. Remember: it's a theoretical concept of proportionality. A high Vd just means "the drug prefers to be in the tissues rather than in the blood."
- Mixing up Enzyme Induction and Inhibition: This is a classic mistake with serious clinical consequences. Inducer (e.g., rifampicin) = more enzyme = more metabolism = less effect of the other drug. Inhibitor (e.g., fluconazole) = less enzyme = less metabolism = more effect and toxicity of the other drug.
- Not understanding Zero-Order Kinetics: Students memorize the examples (phenytoin, ethanol) but not the implication: at therapeutic doses, small dose increases can cause disproportionate rises in plasma concentration and toxicity because the elimination system is already saturated.
Is Your Exam Different?
This quiz covers the pillars of pharmacokinetics that every medical student must master. These are universal concepts.
However, your exam wasn't designed by a blog. It was designed by your professor. And every professor has their favorite topics, trick questions, and specific clinical examples they've repeated in class. Maybe they focus more on flow-dependent hepatic clearance, or how renal failure affects the dosage of certain antibiotics. Those questions, the ones that make the difference between a pass and a top grade, aren't on a generic internet quiz.
They're in your notes.
The only way to prepare for THOSE questions is by studying with YOUR material. Upload your Pharmacokinetics (ADME) PDF to Smartests and let our AI analyze your slides, transcripts, and summaries to generate a custom exam, 100% tailored to what you'll be asked.
Quick Summary
Today we've tested and reinforced three key ideas:
- A drug's journey through the body (ADME) determines its concentration at the site of action and, therefore, its efficacy and toxicity.
- Quantitative parameters like Vd, Clearance (Cl), and Half-life (t½) are interconnected and allow us to predict a drug's behavior.
- Interactions (like enzyme induction/inhibition) and patient conditions (like urinary pH) can drastically alter pharmacokinetics, making them a critical point in clinical practice.